
On April 30, 2024, the news leaked that the Biden Administration plans to reschedule marijuana from a Schedule I drug to a Schedule III drug. The Administration will soon initiate a Notice of Proposed Rulemaking (NPRM) which means the public will have the opportunity to comment. The comments submitted are considered part of the official record and the Administration is supposed to take public comments into account before issuing a final rule. After the public comment period is over, the Administration will examine the comments and issue a final rule. If the Administration decides to move marijuana to Schedule III, then SAM is prepared to pursue legal action.
Click here to contribute to SAM’s rescheduling legal fund
On August 30th, 2023, the Department of Health and Human Services (HHS) announced it recommended the reclassification of marijuana from Schedule I to Schedule III to the Drug Enforcement Administration (DEA). HHS’ recommendation sends the wrong message about marijuana, saying that it is less likely to be addictive, which we know is not true, as well as giving the industry an easier path to being legitimate. Schedule III also gives the industry access to certain tax advantages which will allow these companies to write off their business expenditures on their taxes. This could include things like advertising, which is concerning because of the industry’s track record.
Drug scheduling is not a harm index
The scheduling of drugs is not a “harm index” or directly used to determine criminal penalties for drugs. Scheduling is not synonymous with the danger of a drug. Rather, it is a technical legal term that categorizes drugs according to their potential for abuse and accepted medical value. Marijuana meets the technical definition of Schedule I because it has a high potential for abuse and has no FDA-approved use.
{kind=link}
Resources
SAM’s Press Statement on DEA’s proposed rescheduling (May 2024)
SAM’s Press Statement on DEA’s proposed rescheduling (April 2024)
Talking Points (Updated April 2024)
SAM’s Analysis of HHS’ Recommendation
Kevin Sabet in Newsweek: Proposed Marijuana Rescheduling Doesn’t Follow the Science
SAM Statement: Bipartisan Group of White House and DEA Heads Urge Biden Administration to Reject Rescheduling of Marijuana
Letter: Former ONDCP Directors and DEA Administrators Urge Biden to Reject Rescheduling
SAM Statement: Bipartisan Coalition of Former U.S. Attorneys Urge DOJ, DEA to Reject Marijuana Rescheduling
Letter: Former U.S. Attorneys Urge DOJ, DEA to Reject Rescheduling
SAM Statement in Response to HHS’ Recommendation (August 2023)
SAM Webinar: Rescheduling of Marijuana (June 2024)
Frequently Asked Questions
Marijuana Rescheduling Public Comment Process:
How long do I have to comment?
The 60-day comment period ends on July 22, 2024; you must submit your comment before then.
Who can read my comment?
The comment you submit will be a part of the public record and will be visible to the public. Do not include any information in the comment that you do not want made public.
Why is it important for me to comment?
The comments submitted are considered part of the official record and the Administration takes public comments into account before issuing a final rule. After the public comment period is over, the Administration will examine the comments and issue a final rule. You can impact this process!
Does my voice matter?
This decision is not a foregone conclusion! The DEA said in the proposed rule: “DEA has not yet made a determination as to its views of the appropriate schedule for marijuana.” Not only that, DEA’s argument is crafted in a way that indicates they see the rationale for rescheduling as lacking a strong basis. The public comment period represents the best opportunity for our movement to make the case that marijuana belongs in Schedule I.
Why is it important to get as many people as possible to comment?
While these rules aren’t weighted based on the number of positive and negative comments, the Administration can take the total number of positive or negative comments into account when issuing a final rule. There is no doubt the other side will flood this rule with positive comments, so please spread this far and wide to anyone you know who is opposed to the legalization of marijuana.
What can I add to this discussion?
We want to point out ways that rescheduling marijuana and making it more available would impact society. Your unique perspective, whether it’s related to your area of expertise or your lived experience, can help the DEA understand why marijuana does not belong in a less restrictive schedule. Please personalize your comment and include information on how this schedule change would impact you personally or would impact your career field.
Should I just submit what is provided?
You are welcome to submit what we have provided, but it is better to add your own language (even if it is just one sentence!). However, if you’re not sure what to say, submitting what is provided is fine.
What else is SAM doing on this?
SAM is preparing an organizational comment and is helping solicit feedback from researchers and experts in this field. With the assistance of our legal team, we are working with a coalition of partners to put forth the best possible argument to defeat this decision. If you are an expert in science or medicine or a leader who would be interested in submitting expert testimony, please reply to this email and we will be in touch. If you would like to contribute to our legal efforts on this issue, please click here.
Marijuana Rescheduling Process:
What determine’s a drug’s Schedule?
The Controlled Substances Act (CSA) places all substances which were in some manner regulated under existing federal law into one of five schedules based upon the substance’s medical use, potential for abuse, and safety or dependence liability. Schedule I drugs are determined to have a high potential for abuse and no commonly accepted medical use, Schedule II drugs are determined to have a high potential for abuse but some accepted medical use and so on.
The DEA details each schedule’s criteria here.
Read more about the Controlled Substances Act and scheduling from the DEA here.
How are drugs scheduled or re-scheduled?
Controlled substances can be rescheduled two ways:
- The Drug Enforcement Administration (DEA) conducts a scheduling review and the Department of Justice (DOJ) makes a final determination.
- Congress passes legislation to schedule or reschedule a drug.
What does the drug scheduling process look like?
Considerations on drug scheduling can be initiated by anyone and are reviewed every decade or so. This review was initiated by President Biden in October 2022. The Attorney General directs the FDA to gather relevant scientific and medical information (outlined below), the FDA submits those findings to the AG and makes their recommendations based off of the findings. If the FDA recommends scheduling the drug, the DEA reviews the findings and makes a determination. Then the agency in charge will initiate rulemaking proceedings. There will be a public comment period of 30-60 days where the public can weigh in on that decision. After the comment period is over, the agency must review the comments and craft a final rule with those comments in mind. After the final rule is issued, it is then ripe for any legal challenges and any potential action from Congress.
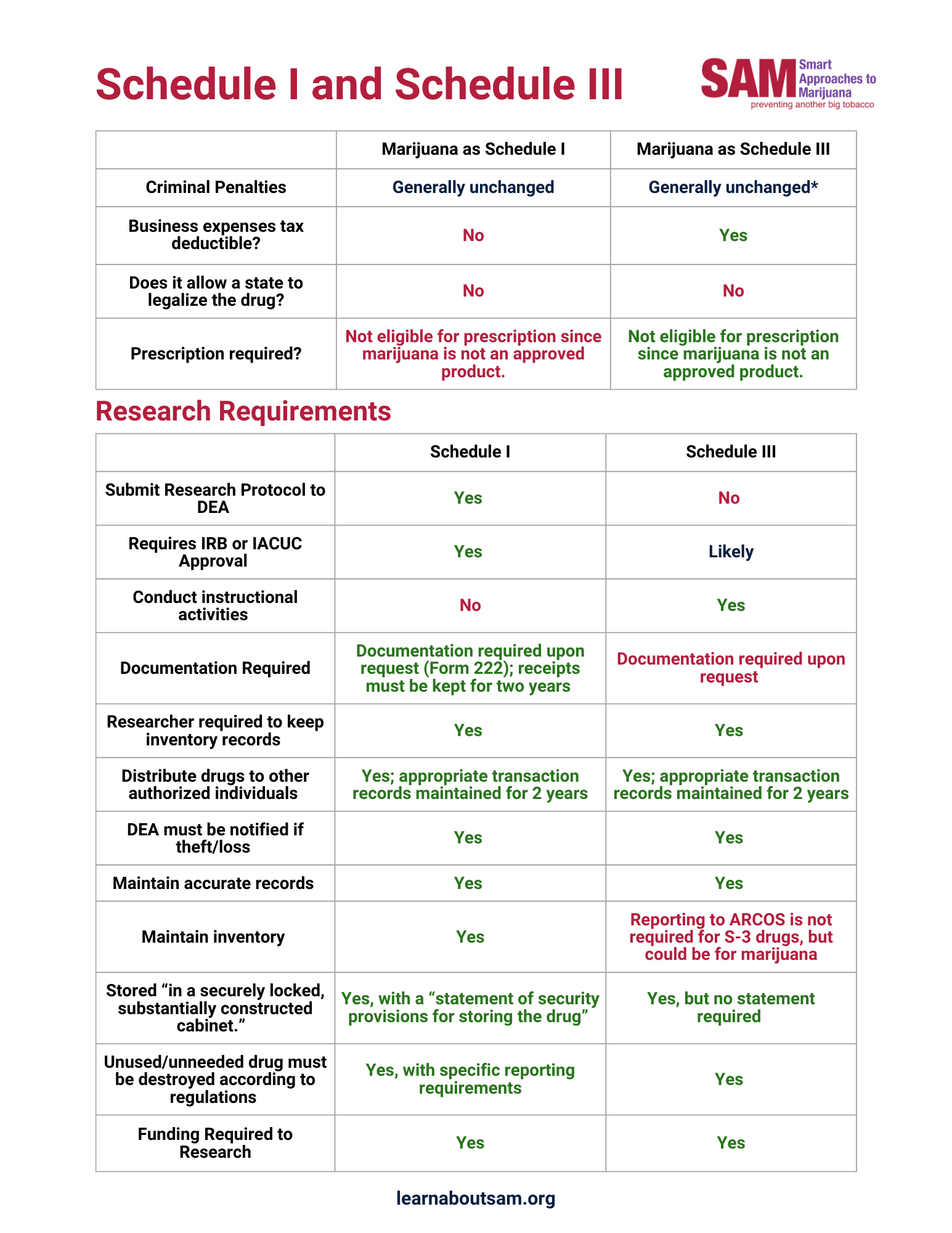
What’s the difference between Schedule I and Schedule III?
Schedule I substances are defined as having no accepted medical use and a high potential for abuse. Schedule III substances are defined as drugs with accepted medical use, meaning they may be prescribed, dispensed or administered; and have a moderate to low potential for physical and psychological dependence.
The most significant difference for the marijuana industry is that Schedule III would allow the industry to deduct ordinary business expenses, as it would no longer be subject to Section 280E of the IRS regulations, which stops businesses from deducting expenses related to the trafficking of Schedule I drugs. This would make the marijuana industry much more profitable.
What other drugs are in Schedule III?
Some depressants (the ones people with a drug use disorder do not usually seek), Anabolic steroids, Buprenorphine, Ketamine, and Codeine, for examples. However, all of these drugs have an FDA accepted medical use/indication for use, marijuana does not.
On what grounds did HHS recommend the change from Schedule I to Schedule III?
HHS’ recommendation is based on cherry-picked data and represents a weak and intellectually dishonest argument to reschedule marijuana. Read SAM’s full analysis of HHS’ recommendation that provides an in-depth analysis of what the HHS got wrong and how the process could have been strengthened.
If marijuana is moved to Schedule III, does this mean marijuana is legal?
No. Marijuana is still federally illegal. Schedule III drugs are still controlled drugs and improper sale or transfer of these drugs carries criminal penalties for trafficking, sale, etc.
What will happen in states with marijuana commercialization if marijuana is moved to Schedule III?
Nothing; these states are still out of compliance with federal law, the activities surrounding marijuana, including banking, are also still federally illegal.
Has marijuana or the science around marijuana changed since the last time the DEA looked at scheduling?
No, if anything, we have more evidence pointing to the potentially addictive nature of marijuana. Read SAM’s analysis of HHS’ recommendation for more information. The DEA’s denial of rescheduling petition from 2016 is still completely accurate.
Is it really fair to put marijuana in same category as heroin and LSD?
The scheduling of drugs is not a “harm index” or directly used to determine criminal penalties for drugs. Scheduling is not synonymous with the danger of a drug. Rather, it is a technical legal term that categorizes drugs according to their potential for abuse and accepted medical value. Marijuana meets the technical definition of Schedule I because it has a high potential for abuse and has no FDA-approved use.
Rescheduling is also a source of major confusion. Rescheduling marijuana – while symbolically important for special interest groups – would not have much of a real-world consequence in terms of reducing criminal penalties. Recreational use of Schedule II drugs is still illegal and can come with significant criminal liability.
Still, we support efforts to increase access to marijuana for research to help the FDA find additional therapeutic uses for the drug. SAM published a six-point plan in 2015 that called for changes such as allowing more licensers to grow marijuana for research purposes, and establishing compassionate research programs for the seriously ill.
Does SAM believe in rescheduling marijuana, to Schedule II or III for example, so that we can study the medicinal benefits of marijuana?
SAM wholeheartedly believes that we need to fast-track the FDA process to extract non-smoked medications from the cannabis plant. SAM also believes that in the meantime, before we have more cannabis-based FDA-approved medications, FDA and HHS should administer a program whereby the truly sick and dying can receive yet-to-be approved, non-psychoactive, non-smoked components of marijuana under a special research program. But rescheduling marijuana is neither necessary nor desirable for those actions to happen.
Rescheduling marijuana would do nothing to allow for more cannabis-based medicines. In fact, cocaine is Schedule II today and is not allowed in a widespread fashion. Rescheduling would simply be a symbolic victory for advocates who want to legalize marijuana.
SAM in the News
SAM in National News
- Dr. Kevin Sabet in The Wall Street Journal: Biden Administration Aims to Reclassify Marijuana as Less Dangerous Drug. Read the rest of the piece in The Wall Street Journal.
- Dr. Kevin Sabet in The New York Times: Justice Dept. Recommends Easing Restrictions on Marijuana. Read the rest of the piece in The New York Times.
- Dr. Kevin Sabet in NBC News: Biden administration plans to reclassify marijuana, easing restrictions nationwide. Read the rest of the piece in NBC News.
- Dr. Kevin Sabet in AP News: Justice Department formally moves to reclassify marijuana as a less dangerous drug in historic shift. Read the rest of the piece in AP News.
- Dr. Kevin Sabet in CBS News: Chicago dispensary operators are pleased about plan to reclassify marijuana, but not everyone is. Read the rest of the piece in CBS News.
- Dr. Kevin Sabet in Los Angeles Times: DEA’s big marijuana shift could be a lifeline for California’s troubled pot industry. Read the rest of the piece in Los Angeles Times.
- Dr. Kevin Sabet in The Washington Post: Democrats hope move to reschedule marijuana will help them in November. Read the rest of the piece in The Washington Post.
- Dr. Kevin Sabet in Reuters: US Justice Department takes step to make marijuana use a less serious crime. Read the rest of the piece in Reuters.
- Dr. Kevin Sabet in Newsweek: Marijuana Reclassification Puts Politics and Profits Ahead of Public Health. Read the rest of the piece in Newsweek.
- Dr. Kevin Sabet in Business Times: DEA to Reclassify Marijuana as Schedule III Drug, Easing Federal Restrictions. Read the rest of the piece in Business Times.
- Dr. Kevin Sabet on CSPAN Washington Journal: Kevin Sabet and Paul Armentano on DEA Plans to Reclassify Marijuana. Watch the video here.
- SAM mentioned in Politico: Biden administration poised to weaken weed restrictions, a seismic shift from decades of harsh policies. Read the rest of the piece in Politico.
SAM in Local News
- SAM mentioned in NBC 6 South Florida: What does the reclassification of marijuana mean? Here is all you need to know. Read the rest of the piece in NBC 6.
- Dr. Kevin Sabet on NBC 10 Philadelphia: Reclassifying Marijuana. Watch Dr. Kevin Sabet speak at 8:50 here.
- Dr. Kevin Sabet on NBC 5 Chicago: As Biden administration moves to reclassify cannabis, here’s how businesses and others will be impacted. Watch Dr. Kevin Sabet speak at 1:06 here.
- Dr. Kevin Sabet in Chicago Tribune: Illinois pot businesses could gain tax benefits, easier loan access under DEA reclassification. Read the rest of the piece in Chicago Tribune.
- Dr. Kevin Sabet in The Providence Journal: The feds may reclassify marijuana. That could be a big deal for RI businesses. Read the rest of the piece in The Providence Journal.
- Dr. Kevin Sabet in WXYZ ABC 7 Detroit, Michigan: How historic reclassification of marijuana could impact states where it’s legal. Read the rest of the piece in WXYZ ABC 7.
- Dr. Kevin Sabet in WALB News 10 Albany, Georgia: State lawmaker speaks on possible reclassification of marijuana. Read the rest of the piece in WALB News 10.
- Dr. Kevin Sabet in FOX 11 News Green Bay, Wisconsin: Marijuana activists, opponents weigh in on potential impacts of DEA’s reclassification. Read the rest of the piece in Fox 11 News.
- Dr. Kevin Sabet in WTKR CBS 3 Hampton Roads Norfolk, Virginia: DEA’s move to reclassify marijuana is ‘significant,’ advocates say. Read the rest of the piece in WTKR CBS 3.
- Dr. Kevin Sabet in The Center Square: Biden’s plan to reschedule marijuana could help investors, but some raise concerns. Read the rest of the piece in The Center Square.
- Dr. Kevin Sabet in MassLive: Feds move to reclassify marijuana: What does it mean for Massachusetts? Read the rest of the piece in MassLive.
- Dr. Kevin Sabet in CBN: Biden Admin to Make It Easier to Access Marijuana, Experts Warn It’s Anything but Benign. Read the rest of the piece in CBN.
- SAM Executive Vice President Luke Niforatos on Mornings on Merit Street: Rescheduling Marijuana. Watch the video here.
- SAM Executive Vice President Luke Niforatos on WHTM ABC 27 Harrisburg, Pennsylvania: Impacts on Pennsylvania if federal marijuana restrictions are relaxed. Watch the video here.
- SAM Executive Vice President Luke Niforatos on NBC 10 Knoxville: Community leaders discuss future of marijuana in Tennessee after federal proposal on reclassifying as Schedule 3 drug. Read the rest of the piece in NBC 10.
- SAM Executive Vice President Luke Niforatos in FOX 10 Phoenix – Marijuana reclassification: How the change in drug laws impacts Arizona. Read the rest of the piece in Fox 10.
- SAM Executive Vice President Luke Niforatos in Fox 43 Harrisburg: Marijuana’s reclassification could have impacts in Pennsylvania. Read the rest of the piece in Fox 43.
- SAM Executive Vice President Luke Niforatos in WKBW Buffalo, New York: U.S. DEA reclassifying marijuana as ‘Schedule 3’ drug calling it a ‘less dangerous drug’. Read the rest of the piece in WKBW.
- SAM Executive Vice President Luke Niforatos in NBC 12 Winston-Salem: Biden Administration announces plans to reclassify marijuana, easing federal restrictions. Read the rest of the piece in NBC 12.
- SAM Executive Vice President Luke Niforatos in Fox 59 (Nexstar): Democrats reintroduce legislation to decriminalize marijuana. Read the rest of the piece in Fox 59.
- SAM Executive Vice President Luke Niforatos on The Lars Larson Show: Federal Changes to Marijuana Policy. Listen to the show here.
- SAM Director of Community Engagement and Outreach Will Jones in Fox 5 DC: DEA looks to reclassify marijuana as less dangerous drug. What does that mean for the DMV? Read the rest of the piece in Fox 5 DC.
- SAM Government Affairs Manager Jordan Davidson in WORLD News Group: The World and Everything in It for May 9, 2024. Read the rest of the piece in WORLD News Group.
SAM in International News
- Dr. Kevin Sabet on ABC News Australia: Planet America’s Fireside Chat. Watch Dr. Kevin Sabet speak at 22:00 here.
- Dr. Kevin Sabet in Japan Today: What marijuana reclassification means for the U.S. Read the rest of the piece in Japan Today.